
Introduction
Why It Matters
How We Find Out
What We Know
Story Time
Common Hazards
Activities
Self-Study Game
Introduction

The whistle blows and practice is over, so you run in from the field. You’re out of breath from all the running you’ve been doing for the past hour. But have you ever wondered what causes you to become out of breath or even why breathing faster seems to help you recover?
When you run, your body uses energy that is taken from the food you eat every day. Cells can only obtain the energy from your food if there is a special gas called oxygen in your body. Oxygen in the air is brought into your lungs when you inhale. Blood picks up the oxygen from your lungs and carries it through the bloodstream to every cell in your body.
Cells use the oxygen and produce another gas, called carbon dioxide, as a waste product. It is very dangerous if carbon dioxide builds up in your body, so your blood carries the carbon dioxide to your lungs where it is released into the air when you breathe out or exhale.
This module will help you understand how gas exchange occurs in the body and why it is so important.
Objectives
After completing this lesson, each student should be able to:- Diagram and label the anatomy of the lungs and the circulatory system.
- Explain how the processes of gas exchange occurs and what purpose it serves.
- Explain the harmful effects that smoking and air pollution have on the body
Why It Matters
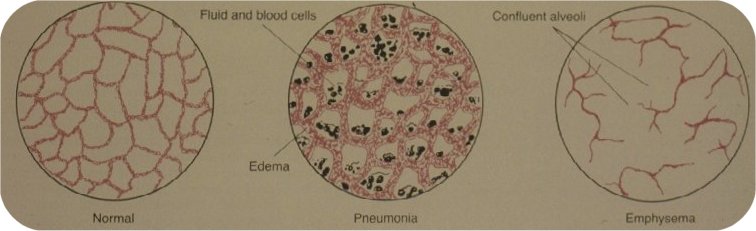 Cross cuts of lung tissue. Normal lung is on the left. Pneumonia (middle picture) is usually caused by infections of the lung that cause the cells lining air sacs to swell (“edema”) and the airs spaces to fill with blood cells, fluid, and cellular debris. Emphysema (right-hand picture) is usually caused by smoking, which breaks down the air sacs, making them lose their elastic properties and keeping them from emptying air properly.
Carbon dioxide gas is a waste product of cells and is toxic if allowed to accumulate in your cells.
If a lack of oxygen or too much carbon dioxide causes enough cells to die, the entire organism would die.
These critical gases have to be transported through the entire body. This is why blood vessels are needed. And the heart is needed to pump the blood and its gases through the vessels. Blood needs to circulate to the cells where it drops off oxygen and picks up the carbon dioxide waste. From there it makes its way to through the body to the lungs where it can come in contact with outside air.
Cross cuts of lung tissue. Normal lung is on the left. Pneumonia (middle picture) is usually caused by infections of the lung that cause the cells lining air sacs to swell (“edema”) and the airs spaces to fill with blood cells, fluid, and cellular debris. Emphysema (right-hand picture) is usually caused by smoking, which breaks down the air sacs, making them lose their elastic properties and keeping them from emptying air properly.
Carbon dioxide gas is a waste product of cells and is toxic if allowed to accumulate in your cells.
If a lack of oxygen or too much carbon dioxide causes enough cells to die, the entire organism would die.
These critical gases have to be transported through the entire body. This is why blood vessels are needed. And the heart is needed to pump the blood and its gases through the vessels. Blood needs to circulate to the cells where it drops off oxygen and picks up the carbon dioxide waste. From there it makes its way to through the body to the lungs where it can come in contact with outside air.
 Some 50 years ago, there was a worldwide epidemic of polio, which caused paralysis. Most victims were children. Some unfortunate children had paralysis of the muscles used in breathing. In order to breathe, they had to spend their life in “iron lungs” such as the one diagrammed above.
The lungs are the place where gas exchange with air takes place (in fish, gills serve the same purpose). Oxygen-deficient blood coming from cells picks up oxygen from the air in the lungs. At the same time, the surplus carbon dioxide is given off to outside air.
Some 50 years ago, there was a worldwide epidemic of polio, which caused paralysis. Most victims were children. Some unfortunate children had paralysis of the muscles used in breathing. In order to breathe, they had to spend their life in “iron lungs” such as the one diagrammed above.
The lungs are the place where gas exchange with air takes place (in fish, gills serve the same purpose). Oxygen-deficient blood coming from cells picks up oxygen from the air in the lungs. At the same time, the surplus carbon dioxide is given off to outside air.
How We Find Out
Today a large number of scientists are working very hard to learn more about the body systems that affect gas transport and the diseases that affect it. Let’s take a closer look at how they discovered the things we know about the respiratory system.
How do we measure breathing?
A spirometer is a piece of equipment that scientists use to measure lung capacity and the amount of air a person normally breathes in and out. You will have an opportunity to make your own spirometer in activity #1.
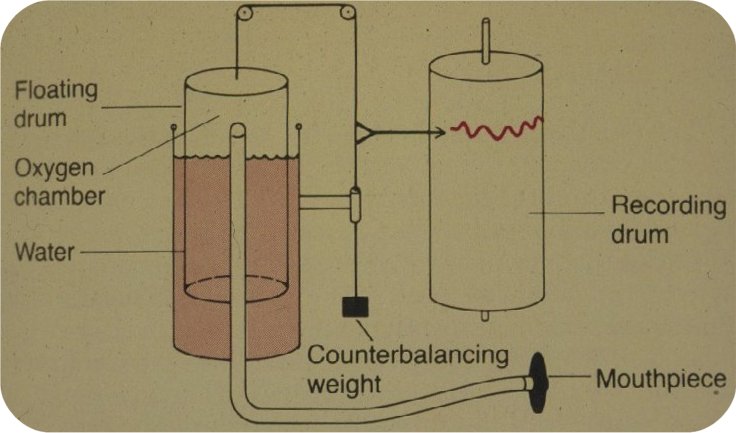
Basic idea of measuring air exchange, using a “spirometer.” As air is taken in (from the “oxygen chamber” in the apparatus on the left), the floating drum drops down. At the same time the writing arm on the recording drum moves up, indicating inhalation. Opposite effects occur during exhalation.
How can you make a good estimate of the amount of air you breathe in a day?
- One way to do this is to multiply the amount of air you breathe in one breath x the number of breaths you take in a minute x 1440, which is the number of minutes in a day.
- Can you think of any other ways?
Every day our body breathes in and out as much as 10,000 liters of air. If we were talking about soda, this would be enough soda to fill 5000 two-liter bottles. 5000 bottles of soda weigh about the same as 11 average size cars. Knowing that a bottle of soda ways about 4.4 pounds and an average size car ways 2000 pounds, can you figure out how to make this calculation? (Answer: To make this calculation multiply the following: 5000 Bottles Soda x 4.4 pounds and 11 Cars x 2000 pounds)
You can make a good estimate of how much air you breathe in and out everyday. To do this observe your breathing rate by counting the number of breaths you take in a minute and use a spirometer to figure out how much air you breathe in during a single breath at rest (about 0.300 liters is average for a 12 to 13 year old).
A spirometer can tell a doctor how far a respiratory disease has progressed and help determine what the treatment should be (See Hazards). One of the more common breathing problems in children is asthma, an allergy disease that causes chronic inflammation and swelling of the bronchial tubes. This limits the amount of air that a person can breathe in and out at a given time.
How do we know how lungs work?

Sometimes the best way to find out how something works is to take it apart and figure out what the smaller parts do. That’s exactly what scientists have done to learn about the lungs. Some people donate their bodies to medical schools after they die, so that doctors can study the parts and try to figure out how they work. Animal studies have also been used to learn about the lungs. Scientists look closely at all of the different parts of the lung including the alveoli, bronchiole, bronchial tubes, membrane linings, and the different lobes of the lung.
In living people, physicians can view the inside of the lung using a fiber optic camera, called an endoscope. Using an endoscope, physicians can observe the lung while it is moving and observe very closely the changes that take place during respiration.
Scientists have also learned about the gas exchange that takes place in the lungs by sampling the air directly. They have learned what makes up inspired air and how it differs from air deep within the lungs. For example, they have learned that when air enters the lung it is greatly humidified in order to facilitate gas exchange. In order to do this, the lung makes the air a bit “thicker” and causes it to stay in the lungs longer, increasing contact time and gas exchange. This is the reason that it is sometimes easier to breathe in a room with a humidifier.
How do we know what happens to the air we breathe?
A simple way of following air through are body is to look at the color of blood. When blood is bright red it means that oxygen is bound to the hemoglobin in the blood. When less oxygen is in the blood, the blood becomes a darker shade of red, very close in color to maroon.

- Most arteries carry oxygenated blood from the heart to the rest of the body. As the oxygen is released into the tissues, the blood slowly turns a darker shade of red and returns to the heart in veins.
- Most arteries will be a pink to reddish color, while veins are a blue or purple color.
- Arteries are thick and muscular. Veins are thin and flabby.
- From dissection of an animal body, you can see where oxygen is going from the heart by following the arteries. You can see where carbon dioxide is leaving by following the veins back to the heart
What you can NOT see (without a microscope) is how arteries are connected to veins.
- The heart has an artery that carries blood to the lungs to pick up oxygen, and release carbon dioxide; this is the only artery in the body that does not have oxygen-rich blood.
- When blood from the heart reaches the lungs, the carbon dioxide leaves the blood much like the carbon dioxide that leaves a coke bottle when it is opened.

How do we know about gas exchange in body tissues?
Scientists measure oxygen and carbon dioxide in various heart chambers and blood vessels. They notice that the big changes in both oxygen and carbon dioxide occur in the small capillaries, because the gas composition is very different between blood entering a capillary bed and blood leaving it. How do the gases get from the blood to the cells in the body?
- As the blood gets closer to its destination, blood vessels get smaller and thinner, until they get so small and thin that gases and other molecules can freely move in and out of the blood stream.
Why do gases move in and out of the blood?
- The idea is similar to diffusion, which we learned about in the Cells Are Us lesson. What this means is that if there is more oxygen in the blood, some will move into the cells that need oxygen.
- The cell is always using up oxygen and needs more from the blood. We know this because we can observe the color change from red to maroon of blood as oxygen is released from the blood to the tissues.
As the cell uses oxygen, it produces carbon dioxide. The carbon dioxide diffuses from the cell into the blood. How do we know this? Scientists have come up with clever ways of measuring the concentrations of gases at these locations.
- For example, to measure the concentration of carbon dioxide, scientists measure the acidity of the blood (carbon dioxide in blood converts to an acid compound.)
- To measure acidity, scientists measure the acidity of the solution with a pH meter.
- The higher the concentration of carbon dioxide, the more acidic the blood is, and the more toxic it is for the cells.
- The enzymes, that make cells work, function best when the cells are not acidic. The further a cell gets from its “optimal” acidity level, the less effective its enzymes become and the more likely the cell is to die.

What We Know
Story Time
 Valentine’s Day is only five days away as this story is being written. On Valentine’s day we think of hearts and love. For centuries, our culture has used the heart as the symbol of love and even of other feelings. Love songs speak of the heart. We speak of “broken hearts.” We even speak of having the “heart of a lion.”
We all know better. All the heart does is pump blood. This notion that the heart is the seat of love and even of the soul goes back thousands of years. William Harvey came along and proved what the heart really does, but old myths die hard. Even when we see the myths for what they are, we still cling to them.
William Harvey was born in Folkestone, England. Not much else is known about his childhood, although it is a good bet that his family was “upper class.” Harvey went to King’s School at Canterbury. When he was 16, he went to college at Cambridge and was awarded a scholarship. Even then, Harvey was interested in eventually training physicians and Cambridge had a special emphasis in that area. After graduating with a B.A. degree, he went to the most famous medical school in Europe at that time, the University of Padua, in Italy. Although he had a degree from Cambridge, his most important preparation for the discoveries he would later make was the two and a half years of training he received under a tutor named Fabricius in Italy. There, he used direct observation of dissected animals to look for the truth.
Harvey received his medical degree from Padua and returned to England and practiced medicine in and around London. Back in England, he quickly established himself as a physician of great competence. He also had great political connections. This was the Elizabethan age, and Harvey married the daughter of the Queen’s physician. Harvey had a huge practice and was physician to many famous people, including Sir Francis Bacon and the Royal family. Harvey also realized his dream of teaching anatomy to medical students. Among the things he taught medical students was the notion that anatomy “deals with the uses and actions of the parts [of the body] by eyesight inspection and by dissection.” In other words, the truth is in the body, not necessarily in the books or in what supposedly learned men tell you.
Valentine’s Day is only five days away as this story is being written. On Valentine’s day we think of hearts and love. For centuries, our culture has used the heart as the symbol of love and even of other feelings. Love songs speak of the heart. We speak of “broken hearts.” We even speak of having the “heart of a lion.”
We all know better. All the heart does is pump blood. This notion that the heart is the seat of love and even of the soul goes back thousands of years. William Harvey came along and proved what the heart really does, but old myths die hard. Even when we see the myths for what they are, we still cling to them.
William Harvey was born in Folkestone, England. Not much else is known about his childhood, although it is a good bet that his family was “upper class.” Harvey went to King’s School at Canterbury. When he was 16, he went to college at Cambridge and was awarded a scholarship. Even then, Harvey was interested in eventually training physicians and Cambridge had a special emphasis in that area. After graduating with a B.A. degree, he went to the most famous medical school in Europe at that time, the University of Padua, in Italy. Although he had a degree from Cambridge, his most important preparation for the discoveries he would later make was the two and a half years of training he received under a tutor named Fabricius in Italy. There, he used direct observation of dissected animals to look for the truth.
Harvey received his medical degree from Padua and returned to England and practiced medicine in and around London. Back in England, he quickly established himself as a physician of great competence. He also had great political connections. This was the Elizabethan age, and Harvey married the daughter of the Queen’s physician. Harvey had a huge practice and was physician to many famous people, including Sir Francis Bacon and the Royal family. Harvey also realized his dream of teaching anatomy to medical students. Among the things he taught medical students was the notion that anatomy “deals with the uses and actions of the parts [of the body] by eyesight inspection and by dissection.” In other words, the truth is in the body, not necessarily in the books or in what supposedly learned men tell you.
Harvey came along during the Renaissance, the “age of enlightenment” when thoughtful people began to challenge old myths and to explore new ways of looking at things. This fresh approach applied to medicine as well as to art and literature. The ancient belief about what the heart did was challenged by Harvey and he devised clever ways to determine what the heart really did and how blood circulates. In those days, medical professionals recognized that there was arterial and venous blood, but they had some primitive ideas otherwise. For example, they thought that blood originated from three places. The liver provided blood for nourishment and growth, the heart provided blood for life itself, and the brain provided blood for sensation and reason. Arterial blood was thought to be “used up,” never returning to its source. These medicine men had the bizarre notion that the heart did not pump blood, but rather sucked it in like a vacuum when the heart relaxed in between contractions. Movement along the vessels was thought to result from contractions of the arteries! They did know that it took air (actually oxygen) to make arterial blood, but they thought the air was transported by the pulmonary veins into the heart. So, you can see how hard it would be to convince such people of our modern notions of blood circulation. That was the challenge that Harvey faced when he finally figured out the truth and published it in 1628.
Some anatomists in that era helped lay the groundwork for acceptance of Harvey’s ideas. Most notable was Vesalius, who showed that the two sides of the heart were separated. Realdo Colombo worked out the connections with the lung and performed experiments showing that pumping of blood occurred when the heart contracted. Harvey performed actual experiments on animals, first on frogs because their hearts were simpler. He noticed that so much blood left the heart in one minute that there was no way it could continually be absorbed by the body and re-made. His calculations proved that the amount of blood pumped out of the body far exceeded the total amount of blood in the body. Thus, blood HAD to circulate! [Illustration of Blood Circulation] Of course, Harvey could not prove by direct observation how circulation continued through the organs in capillaries. But his experiments proved that there had to be very small connections between the arterial side and the venous side of an organ. One of his most famous experiments was in the human, where he put a tourniquet around the forearm. At first, the arm was tied so tight that arterial blood could not enter. The veins looked normal. When the tie was loosened enough to let arterial blood in toward the hand, yet the surface veins were still closed, the veins became swollen, showing that blood had poured into the hand and then moved back up in veins. Harvey also showed that the valves inside of veins were oriented so that they always directed blood back toward the heart. Harvey published his findings in Latin in a book entitled “An Anatomical Exercise Concerning the Motion of the Heart and Blood in Animals.” All learned books in that day were published in Latin. This one, interestingly, was published in Germany, not England (where he was from). In his own words, here is what Harvey gave as the reason for writing the book, “These views as usual, pleased some more, others less; some chide and calumniated me, and laid it to me as a crime that I had dared to depart from the precepts and opinions of all anatomists; others desired further explanations of the novelties, which they said were both worthy of consideration, and might perchance be found of signal use.” The book was an immediate sensation, because it so effectively challenged views that had dated back to the days of Aristotle. Many people do not realize that Harvey was also a pioneer in reproductive science. He argued that humans and other mammals develop from the eggs of females that have been fertilized by sperm from males. Mammalian eggs had never been seen and it was 200 years later that they were. Harvey’s line of thinking was so persuasive that this idea was immediately accepted, although no proof could be demonstrated at that time. Harvey became a very wealthy man. Not only was his medical practice enormously successful, but he profited from the advice he got from his brothers, who were successful merchants. He gave a building and library to the College of Physicians. But his original manuscripts were destroyed when the building burned down in the Great Fire of London in 1666. Toward the end of his life, Harvey became a political outcast, because the King he served so loyally, Charles I, had been executed in a civil war. Harvey was also troubled by his enemies in the medical community. Some physicians in that day had difficulty accepting that they had been wrong. Harvey’s discoveries would require them to abandon long-held views and practices or require them to construct new justification for practices that they could not give up, such as blood-letting. These people considered Harvey to be a “crack pot,” and they tried to ruin his reputation. His medical practice did suffer. Harvey did not bother to argue the matter, although he did write one rebuttal to a particularly obnoxious critic. Harvey let his observations and clear thinking stand on their own merit. Harvey prevailed, even in his own time. ReferencesCurtis, R. H. (1993). Great Lives – Medicine. New York: Charles Scribner’s Sons Books for Young Readers Harrison, W. C. (1967). Dr. William Harvey and the Discovery of Circulation. New York: MacMillan Company. http://www.fordham.edu/halsall/mod/1628harvey-blood.html Modern History Sourcebook: William Harvey www.williamharvey.org/wm William Harvey Medical Research Foundation www.blupete.com/Literature/Biographies/Science/Harvey.htm
Common Hazards
Activities
Activity One
Orientation
This activity is designed to allow students to make a simple device that can monitor respiration. The activity engages the students by having them take real measurements from their bodies.
Build your own spirometer!
Spirometers are used to measure the amount of air that fits in your lungs and how much air you normally inhale and exhale. This is very useful in learning about our bodies and can help doctors determine if we are sick.
To build a spirometer, you will need the following things:
1- 3 liter soda bottle (empty) with cap
1- 2 foot piece of plastic tubing
1- measuring cup with units in milli-liters
1- a bucket or pan that can hold more than 3 liters of water
1- marker
To build the spirometer use the following procedure:
1. Add half a liter of water (500 milli-liters) to the soda bottle using the measuring cup and mark a line with the marker at the top of the water level. Repeat this until the bottle is full. When the bottle is full, put the cap on the bottle.
This is done to put measuring lines on the bottle.
2. Add sufficient water to the bucket or pan to submerge the soda bottle.
3. Invert the soda bottle and submerge it in the bucket, and remove the cap under the water.
We open the bottle underwater to prevent any unwanted air from entering the bottle.
4. Place one end of the tubing into the soda bottle in the water, and leave the other end outside of the water.
This is the tubing we will use to blow into, in order to determine lung capacity.
Remember to place the bottle in the water upside down before removing the cap.
Don’t forget to insert one end of the hose in the bottle after you open the cap underwater
Before you exhale into the tubing, your spirometer should resemble this picture.
To use the spirometer follow this procedure:
1. While a partner holds the bottle to keep it from flipping over, inhale normally, then exhale the air normally into the tubing connected to the spirometer. Be sure not to blow out all the “extra” air in your lungs. Make a good estimate of the amount of air you exhaled, remembering that each line on the bottle represents a half liter, starting from the top down.
Write this number down, it is your “tidal volume.” The tidal volume is the amount of air that you normally breathe in and out.
2. Refill the bottle with water and reinsert the tubing. While your partner holds the bottle, take a few normal breaths to help get a good reading on this next step, and then inhale as much air as you can and exhale this air into the end of the tubing outside of the water. Make a good estimate of the amount of air you exhaled by looking at the lines on the soda bottle.
Write this number down, it is your “inspiratory reserve.” The inspiratory reserve is the amount of air that your lungs can hold in.
3. Refill the bottle with water and reinsert the tubing. While your partner holds the bottle, take a few normal breaths to get yourself back to a normal breath, and then exhale as much air as you can into the end of the tubing outside of the water. Make a good estimate of the amount of air you exhaled by looking at the lines on the soda bottle.
Write this number down, it is your “expiratory reserve.” The expiratory reserve is the amount of air that your lungs can blow out after a normal breath..
How much air can my lungs hold?
If the “inspiratory reserve” and the “expiratory reserve” and the “tidal volume” are added together, then you get the “vital capacity,” or the functional capacity of the lungs. The vital capacity is the greatest change in volume that can occur in the lungs. This is not the total volume of air that fits in the lungs, but it is a good approximation.
Inspiratory Reserve + Expiratory Reserve + Tidal Volume = Vital Capacity
Activity Two
How about an adventure inside the human body? Try this virtual endoscopy.This is an external linkActivity Three
OrientationThis activity is designed to allow students to examine the impact of smoking. Students should use information from this unit as well as other resources to find the answers.
Answer the following questions! 1. Why is smoking hazardous?
2. Do “snuff” and chewing tobacco contain nicotine? What about irritants and carcinogens? Are these hazardous?
3. What is meant by “addiction”?
4. Are cigars and pipes more hazardous than cigarettes? Why or why not?
5. Can you reduce the chance of lung diseases? If so, how?
6. Why do some scientists believe that secondhand smoke is more dangerous than smoking a regular cigarette?
7. Does cigarette smoke contribute to air pollution? If so, How?
8. How does smoking change the way the body works? Is this good or bad?
Activity Four
OrientationThis activity focuses on measuring respiratory values. By measuring lung capacities and respiratory rates, the students will use the resulting data to first predict, then test their hypothesis. Various graphs can be charted from the results giving students the opportunity to practice graphing different types of graphs, as well as gleaning conclusions from the data analysis.
Materials
1 balloon for each student
Flexible measuring tape
Measuring stick/Ruler
Lung Capacity Data Sheets
Student Journal
Measuring respiratory values not only helps us understand how the lungs work, but it also can help doctors determine if a patient might have lung disease. In this activity, we will measure vital capacity using balloons and then compare these values to our fellow classmates. Vital capacity is the volume of air that can be expelled after a full inhalation. The total air holding capacity of the lung is the sum of the vital capacity and the residual volume. Even when you try extremely hard to expel all of the air in your lungs, there is still some air left in the alveoli and airways. If there wasn’t, then your alveoli and airways would collapse!! If you would like to make your own spirometer to measure vital capacity, see Activity 1 of this module.
Sit down and take deep breaths in and out five times.
Breath in, as deeply as possible.
Hold a balloon to your mouth, tightly sealing the opening, and blow all the air out of your lungs.Take the balloon out of your mouth, taking care to keep the opening sealed tightly.
Continue holding the balloon while your partner measures the girth of the balloon (in centimeters). The girth is the circumference of the widest part of the balloon. Record this value down on TABLE A as the Vital Capacity Girth. Breathe in and out normally. Have your partner count the number of breaths you take in 30 seconds. (1 breath = breathing in and then out). Double this number to obtain the breaths taken in 1 minute and record this number on TABLE A as the Resting Respiratory Rate. With your partner timing you, run in place for 1 minute. At the end of one minute, sit down to have your elevated respiratory rate measured. (Partner: As soon as the student sits down, measure the number of breaths the student takes in 30 seconds.) Double this number to obtain the breaths taken in 1 minute and record this number on TABLE A as the elevated respiratory rate. Measure your partner’s height in inches and record his/her height and gender on TABLE A. Record your values, and use your values from TABLE A to fill out TABLE B.Activity Five
This is a worksheet for gas exchangeActivity Six
OrientationThis activity is designed to allow students to get a feel for what it must be like to have asthma.
Materials:
A drinking straw for each student Procedure:
1. Breathe normally for 1 minute and think about what your breathing feels like.
2. Clamp both nostrils shut with thumb and forefinger, and breathe through the straw. Do not open mouth, but make all air move through the straw. Think about what it feels like. Resume normal breathing when it becomes uncomfortable breathing through a straw. Describe the results to a lab partner.
Explanation:
The basic problem in asthma is that the small breathing tubes in the lungs, called bronchioles, become constricted as a result of allergic reactions serving to make the circular muscles around the bronchioles constrict. The narrowing of the air passages is like breathing through a straw. The breathing tubes are not large enough to move all the air that the body needs.